Hi all, I would like to firstly introduce myself. My name is Chris Skitt and I am the physio who is on hand as part of the UKRunChat team for help, advice and suggestions. I have a physiotherapy and health and wellness centre covering Shropshire as well as working in elite football for Shrewsbury Town FC and have nearing 10 years of exeperience.
I will be posting regular blogs over the coming months on selected issues across the running spectrum. I will try to keep my blogs as ‘jargon free’ as possible and try to present the facts as they come. What I would say at this point is unfortunately physio is not one size fits all, so some of the suggestions that I make within my blogs may not suit you individually, it is not the aim to cure all on these blogs but to hopefully provide information that you may be able to relate to. Surprisingly, unlike some think, we are not physioterroists and we don’t enjoy inflicting pain routinely. Therefore, I would suggest that if you are in pain, please find your local physio and make use of them.
So over to the first topic, and im sure an area of the body which many, if not all of you have experienced pain in at some point……the knee.
Within this first blog, I will provide a brief overview of the anatomy of the knee and look to correct some of the myths and mystery that is often placed around the knee and hopefully allow you to understand why the knees can often be so troublesome.
So, the knee……. The middle of the lower limb, this is formed of 3 bones: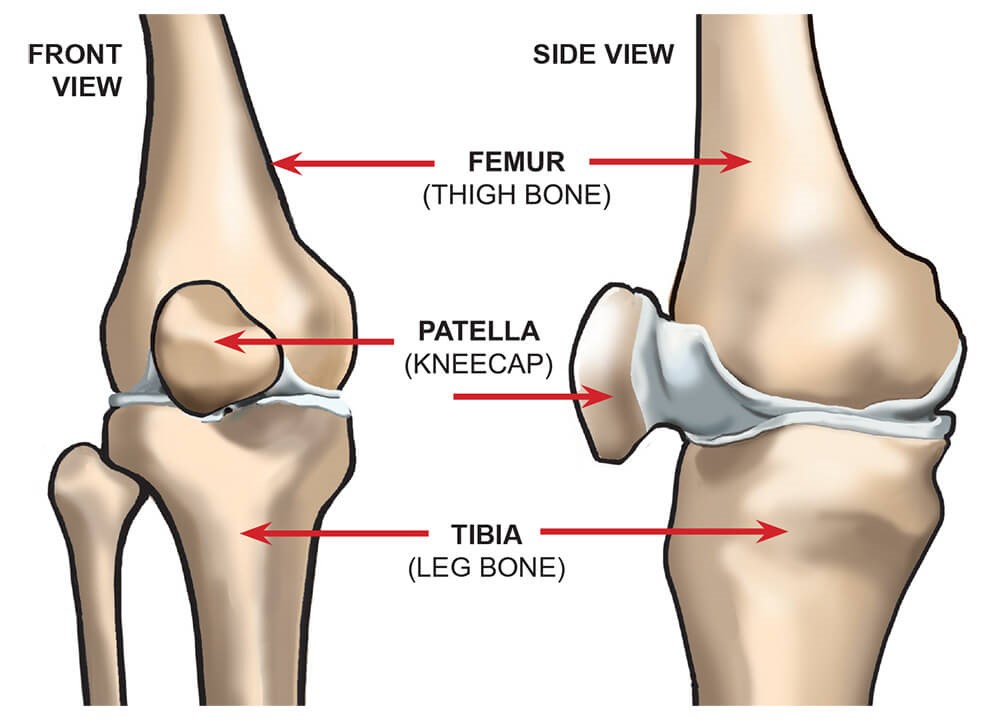
• Tibia
• Femur
• Patella
The knee is classed as a synovial joint because of it being freely moveable and surrounded by a joint capsule. It is further classed as a uniaxial joint, meaning it can only move through one plane of movement, despite having the ability to rotate slightly.
The proximal tibia-fibula joint is sometimes a site of pain which patients feel is part of the knee. Although not strictly ‘the knee joint’, the proximal tib-fib joint has a close relationship to the true knee joint and shares many soft tissue attachment sites.
The tibia and fibula sit end to end with one another and are shaped so that there is a natural congruence with on another. On the front side of the femur (thigh bone) there is a grove, which allows the patella to sit within allowing an articulation to slide up and down efficiently. Each bone ending is covered with a thin layer of hyaline cartilage (sometimes called articular cartlidge), this protects each bone from getting damaged and allows smooth movement.
Where all of these bones meet and forms the strongest joint in the body, there are two wedge shaped tough fibrous structures that serve to provide shock absorption to the knee, so the bones are not damaged during high impact sports, running for example. These two structures are called the meniscus, one on the inside of the knee running from front to back (medial meniscus) and one that runs identical on the outside (lateral meniscus). As I mentioned above, the synovial nature of the joint means that there is a oily capsule that surrounds the knee to provide more shock absorption and protection. This is often the case why knees can swell, because the fluid stays within the capsule and fills like a water balloon.
Around the knee, there are four major ligaments that looks to protect against extreme movement.
Anterior Cruciate Ligament – Situated within the knee joint running from femur to tibia restricted excessive forward translation of the tibia.
Posterior Cruciate Ligament – Works opposite to the ACL and prevent backwards movement of the tibia – this is often damaged in car crashes and is called dashboard a injury
Medial Collateral Ligament – attaches to the tibia and femur and prevents the knee moving excessively side to side.
Lateral Collateral Ligament – On the opposite side of the leg (outside) and provides the opposite support to knee as the MCL.
Within and around the knee joint there are also a number of small layers of padding as well as ‘fatty’ cushions which evolution have placed in strategic positions to protect against excessive forces being transmitted through the joint. These are called fat pads and bursa, the picture below illustrates how many bursa are around the knee.
Ok, so at this point, I hope ive not confused the hell out of you and that you have now got a better grasp of the basics of the knee joint.
Now the important bit, which should hopefully pull everything together for you. There are over 25 individual muscles that run through or attach into the knee. So despite the strength of the ligaments and bones we have already identified, it is the performance of these muscles that really matter!!!!
The huge amount of muscles that run through the knee in some form or other are there for stability or mobility purposes, sometimes even both simultaneously. The aim of these muscles are to of course move the knee to allow tasks that we all love, running for example. To ensure that the knee is working efficiently the muscles also have to perform together to allow the knee to be kept in the plane of movement it was intended to be in (forwards and backwards).
The key muscle groups of the knee are as follows
• The quads – Look to straighten the knee and provide stability in a straight line
• The hamstring – Help to flex the knee which is crucial in the running mechanism
• The groins – Have a huge stability factor and again help to keep the knee along a straight line of work.
There are of course other muscles around the knee that are crucial but extend past the scope of this blog.
So what on earth do all these muscles, ligaments and bones mean anything to us running folk. In actual fact, it is more important than what we think. Think about this analogy, if you are driving a car with the handbrake on, sooner or later there is going to be damage to the car as well as the consistent poor performance. This is exactly what goes on with the knee. If the knee is being loaded in a different way than what it wants to do, there will be compression of the meniscus and other structures as well as over loading or tightening muscles.
A classic example of this in our runners world is iliotibial band syndrome (or runners knee). This is an overloading issue of the iliotibial band, which attaches on the outside of the knee and is responsible for a huge amount of people missing time from running or even dropping out. The correction for this is simply looking to get the knee in a better position by training muscles that affect the position of the knee (the glutes and the inside muscle of the quads primarily) as well as off loading those that are pulling it out of position (ITB).
This is again true with people who are more experienced in the age department. As the knee gets older, there is understandably wear and tear within the knee. Once again, many people then start to experience pain from this degeneration. Unfortunately, once there is damage within the knee it cannot it be fixed, but what you can do ensure that the knee with working as efficiently as possible to keep the knee in a straight line and therefore reduce any poor loading of the knee. This as a consequence, tends to significantly remove the pain that is being experienced, despite the damage still being present
There are a lot of fallacies out there which say, ‘don’t run on the road you will damage your knees’ or ‘if you are a heavier person running will damage your knees’. Quite simply, these are untrue. In both cases, you will experience greater loads going through your knee, but this is the exact reason why you have to ensure that your musculature around the knee are performing to its maximal potential. Also, if you are bigger, and you run………you should lose a bit of weight to which will help
The top tips
• Keep your knees strong by completing strength exercises as well as your running – ie squats and lunges.
• If your knee is sore whilst running you may be suffering from an imbalance within your knee so therefore look to strengthen as well as increase the mobility of your muscles with stretching
• Overactive or tight ITB’s can cause significant pain and restriction of the knee, keep your glutes active and your ITB’s rolled to balance the knee.
• Try to ‘mobilise’ your knee cap regularly to keep it freely moveable and avoid getting restricted movement (It really is as easy as wiggling it about in all directions).
• If you do have pain in your knees when completing your run, ice is often very helpful, it reduces any inflammation within the knee which in turn reduces pressure within the capsule.
I hope you have found this information useful and I also hope that it has given you a little bit more of an insight to the knee. As I mentioned, if you have any questions please do feel free to get in touch or if you have any particular requests for subjects please give me a shout.
Please feel free, to follow me on twitter and like my facebook page for more information.
@CSPhysio_
@csphyzz
www.cs-physiotherapy.co.uk

